What hospital CIOs tell us is broken
14 systems, 1 patient
OPD on one app, IPD on another, pharmacy on a third, lab on a fourth. Nothing reconciles. Doctors hate the logins.
Multi-facility is duct-taped
Two branches, two databases, two billing teams. Cross-branch reporting is a CFO Excel exercise once a quarter.
NABH audit is a fire drill
Audit logs scattered, paper consents, no append-only history. Every assessment costs weeks of prep.
International patients fall through cracks
Medical-tourism inquiries live in WhatsApp; visa letters typed in Word; commission tracking is a spreadsheet.
What enterprise customers get with Medixar Hospital tier
OPD + IPD on one record
- Single longitudinal patient chart across visits, admissions, surgeries, and follow-ups.
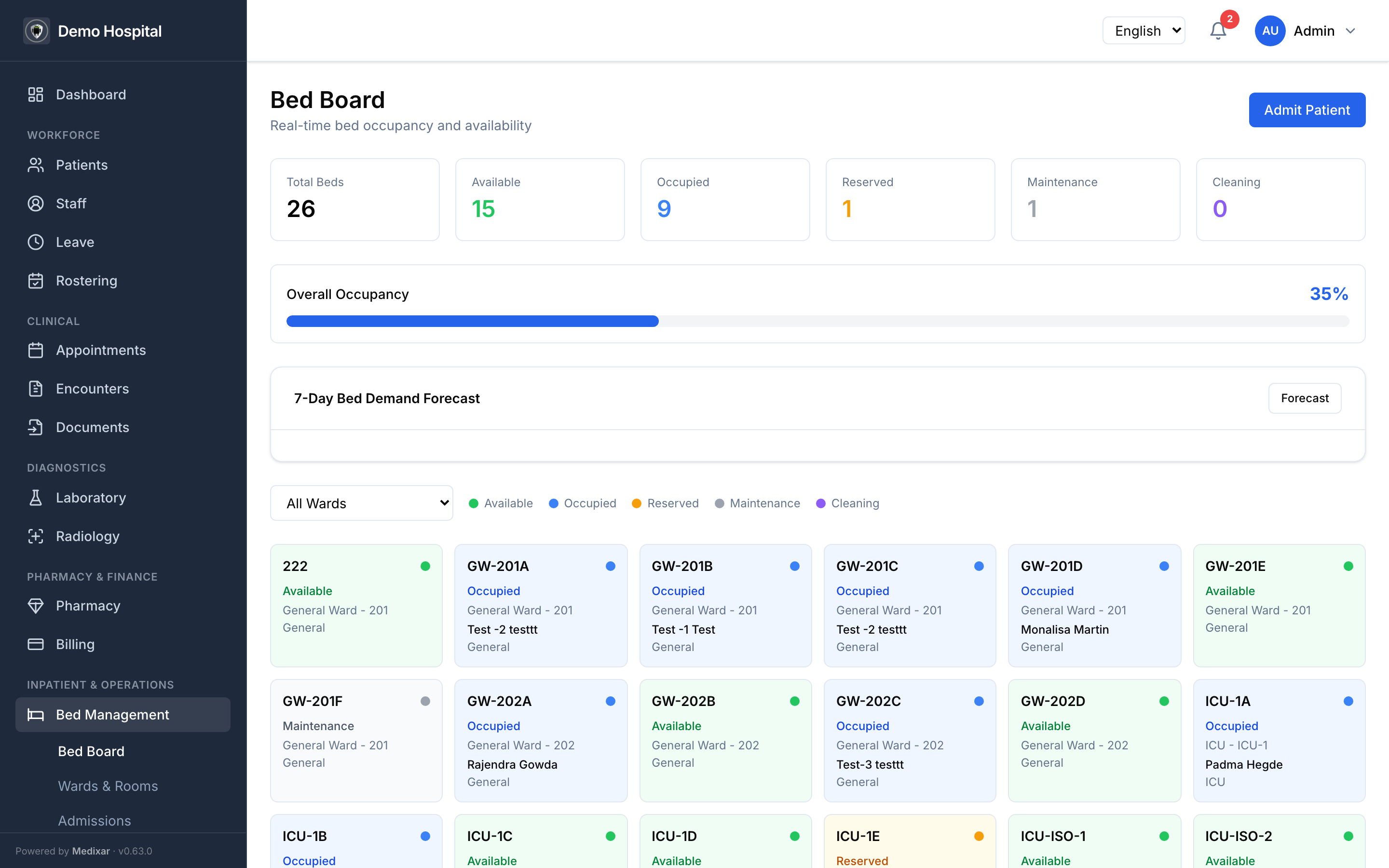
- Bed management with real-time occupancy, transfer, and ward-level demand forecasting.
- MAR (medication administration record) with BCMA + double-check on high-risk medications.
- Operating theatre scheduling, anaesthesia, post-op orders.
- Clinical workspace v2 — autosave per section, finalize-with-co-sign, append-only amendments.
Multi-facility / chain management
- Per-facility KPI dashboards + side-by-side comparison.
- Cross-facility patient search.
- Consolidated revenue + per-facility P&L.
- Staff floating assignments across branches with approval workflow.
- Inventory transfer between branches with audit chain.
AYUSH
- All seven AYUSH systems supported — Ayurveda, Homeopathy, Unani, Siddha, Yoga, Naturopathy, Sowa Rigpa.
- Prakriti / Mizaj / Mukkutram / Nyepa assessments with system-specific consultation surfaces.
- Cross-pharmacopoeia interaction safety with fail-loud partial-failure handling.
- Bhasma batch tracking for NABH-AYUSH compliance.
- Per-system tenant toggles — turn on only the systems you practise.
Medical tourism
- 11-state inquiry pipeline from first touch through post-discharge follow-up.
- FX-locked quotes; visa letters with bilingual templates for 8 corridors (AE / BD / IQ / NG / KE / ET / UZ / RU).
- Interpreter scheduling with overlap protection.
- Commission ledger with append-only state transitions.
- International insurance verification with separation-of-duties workflow.
Billing & revenue cycle
- GST split (CGST + SGST or IGST) decided automatically by patient state.
- Insurance claims with end-to-end submission, status, and remittance posting.
- EDI 835 remittance import.
- Payment plans, write-offs, refunds — all auditable.
- Payment-gateway webhook signature verification + idempotency.
Compliance & audit
- HIPAA §164.312(b)-aligned PHI access audit on every clinical read.
- Append-only audit log at the database level — even our engineers cannot retroactively edit.
- "Break-the-glass" emergency access with privacy-officer review queue.
- ABDM / ABHA verification, consent artefacts, HIE callbacks.
- Daily encrypted backups; 4h RTO, 5-min RPO, restore-tested.
SLA & support
- 99.9% uptime SLA on Hospital tier (99.95% available with signed enterprise contracts).
- Dedicated customer-success manager.
- White-glove onboarding — data migration, staff training, custom integrations — included.
- BAA available; security questionnaire + DPA on request.
- Penetration-test summary available under NDA.
Recommended plan
The Hospital tier (₹24,999/month, up to 50 users) is the right starting point for 50–500 bed facilities. Larger deployments — 500+ beds, multiple branches, or specialised regulatory requirements — get a tailored Enterprise quote.